

We are in the middle of a shut down because of a dispute about federal healthcare spending. The immediate issues are important to millions of Americans: most of the 24 million Americans on Obamacare will face massive increases in their insurance premiums unless a compromise is achieved.
As important as this issue may be, the fact remains that the current American health care financing system is broken. We have a complicated system that does not provide universal coverage that has resulted in very high costs, unequal access and poor outcomes. We can do better. To be clear, Obamacare was a huge achievement that resulted in millions receiving coverage, but the cost, access and outcome problems persist.
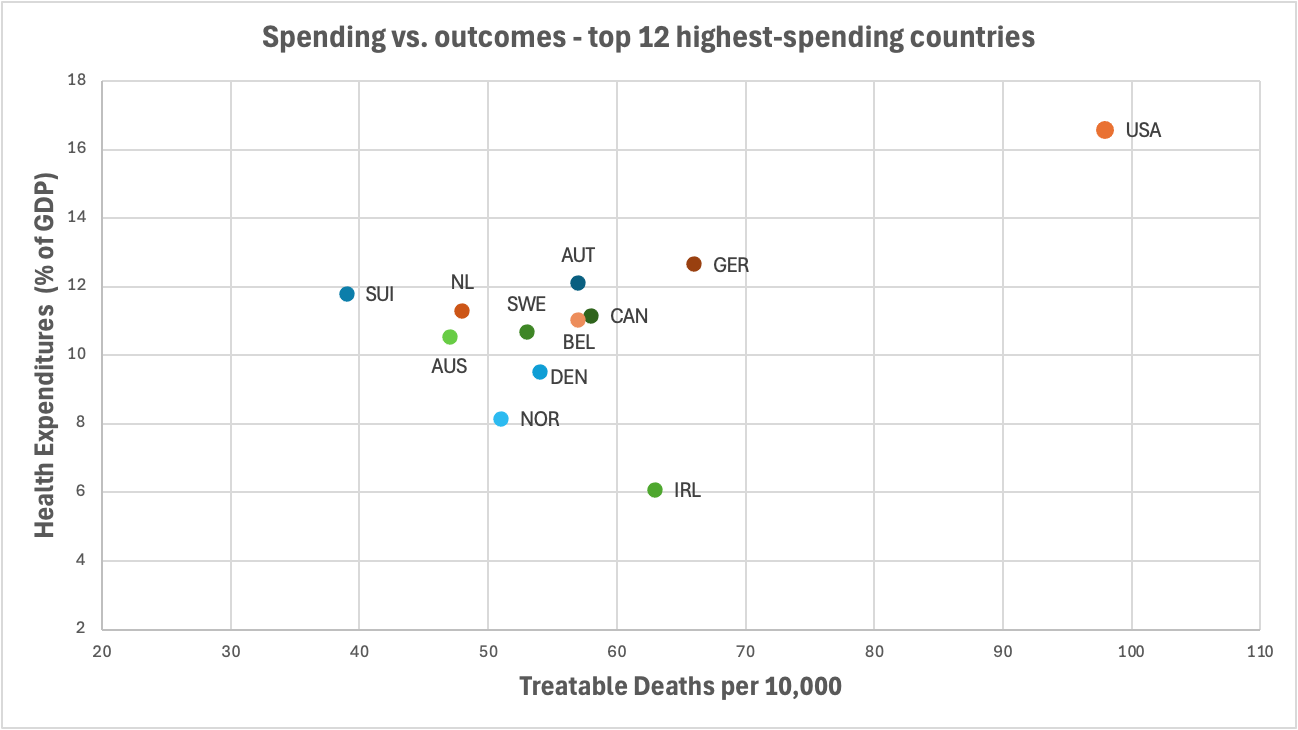
As this chart from the Niskanen Center shows, we are an outlier compared to other countries in both how much we spend on healthcare and our healthcare outcomes. We are far more expensive and get worse outcomes. And the higher costs are a large contributor to our growing national debt.
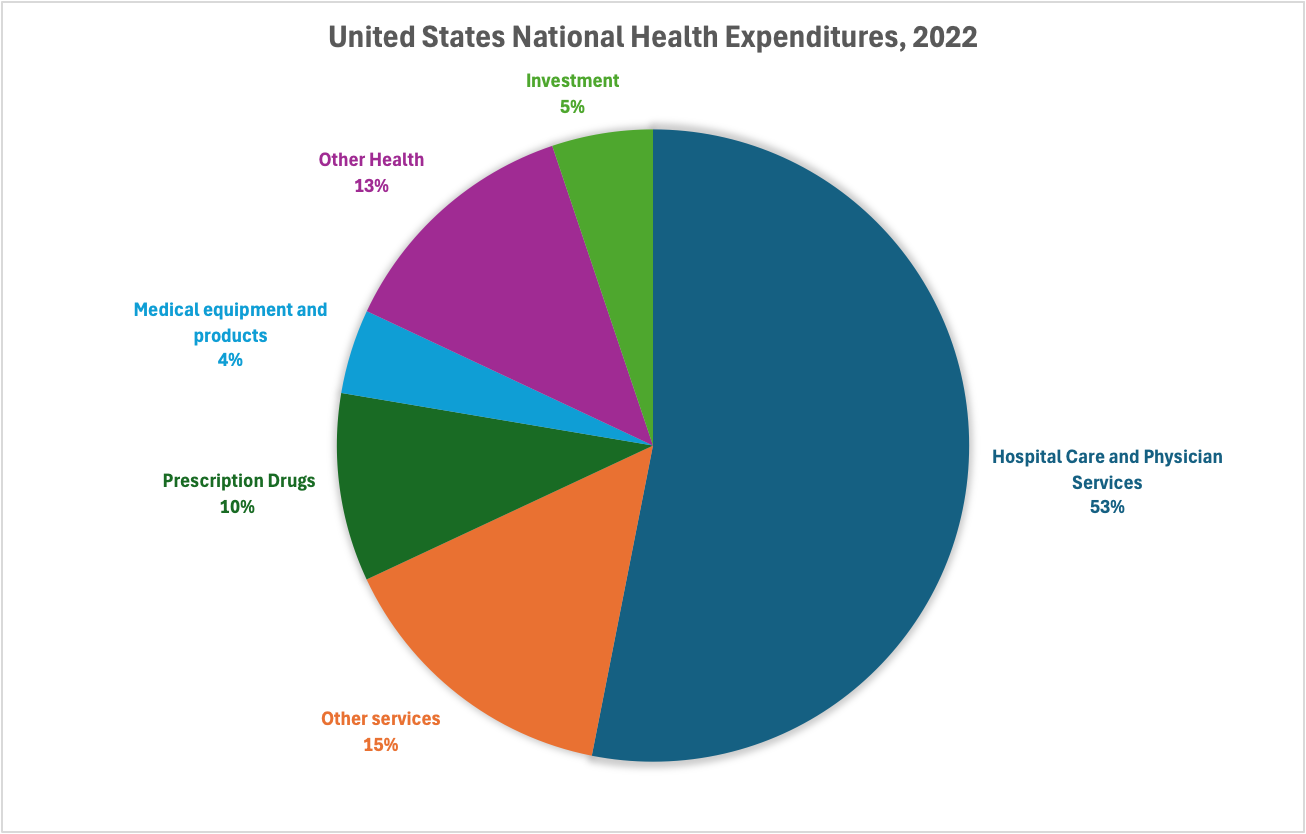
In recent years, our political system has focused on the cost of prescription drugs, but as the chart above shows, drug cost are only a small part of the cost problem—the majority of cost comes from providers and hospitals.
The left advocates for a single-payer system such as those in other countries. The Sanders “Medicare for All” (a misleading title) has the federal government paying all healthcare expenses with no co-pays or deductibles. As attractive as this may be, it has significant downsides. Zero co-pays and deductibles will likely result in much higher costs, not less, because of increased demand for services unless there is a sharp reduction in the incomes of doctors. It also places the decisions about what treatments will be covered in a single entity. In countries with single-payer systems, this means that new treatments only become available years after they are available in the U.S.—and sometimes never. The result is that while the U.S. overall has worse healthcare outcomes than other countries because of access problems , we do much better successful outcomes in treating many diseases. According to a Commonwealth study, we have much higher survival rates for those hospitalized for heart attacks and strokes, and those treated for the most common types of cancer. The study also found that we appear to do a better job managing hypertension and cerebrovascular disease. In short we have the highest quality medical treatment in the world, but one not accessible to all.
I also think true single-payer systems run against the American grain by removing choice. As we saw with the initial role-out of Obamacare, American demand choice. As any senior knows, even the Medicare system gives recipients lots of choices—Medicare Advantage or Original Medicare, numerous private Medigap Options and numerous drug plan options. I don’t think removing choice will fly politically. I also don’t think it is a good idea. Choice gives consumers the ability to reward good performers and punish poor performers. In making my own insurance decisions, I will change companies if the price increases are too high or the service is too low. A true single payer system means we have no choice—and the single payer has no incentive to provide good service.
To me, therefore, the big question is this: are there alternatives to “Medicare for All” that provide for universal coverage at affordable costs for both individuals and the country that still incentive innovation and high quality treatment and maintain consumer choice? In looking at this issue, I found an interesting proposal by the Niskanen Center, a libertarian think tank that has been embraces by centrist think tanks as well.
The proposal, by Niskanen Center economist Ed Dolan, is to have the federal government provide universal catastrophic coverage for all, but leaving payment of healthcare costs below a high deductible to individuals (who may or may not decide to insure). Out-of-pocket expenses for premiums, deductibles and co-pays would be capped on a sliding scale based on income. The truly poor would not have to pay for healthcare, while the deductible for high income Americans could be very high. As with Obamacare, preventive care could be included with no co-pays or deductibles. As Dolan notes, there are lots of challenging policy trade offs to be made in setting the premiums, deductibles, sliding scale details, and co-pays, but the result would be full protection of all Americans from high medical expenses, while still using market incentives to control costs. Consumers would have lots of options to finance health care below the deductible and out-of-pocket maximums—insurance (whether provided by employers or the individual market place), self-insurance, or Health Savings accounts.
Under one proposal, for example, the deductible would be set at 10% of income (with lower percentages below the poverty line) and maximum out of pocket cost would be capped at 14.5% of income. A household with an income of $200,00 would have a deductible set at $20,000 and a maximum exposure of $29,000.
Could we afford such a system? Jodi Liu of the RAND School of Public Policy did an interesting economic analysis of three different healthcare financing systems—Sanders “Medicare for All”, the current Obamacare system, and one set of universal catastrophic coverage—and found that the latter was the least expensive proposal.
Here are the details for the two alternatives to Obamacare that she analyzed:
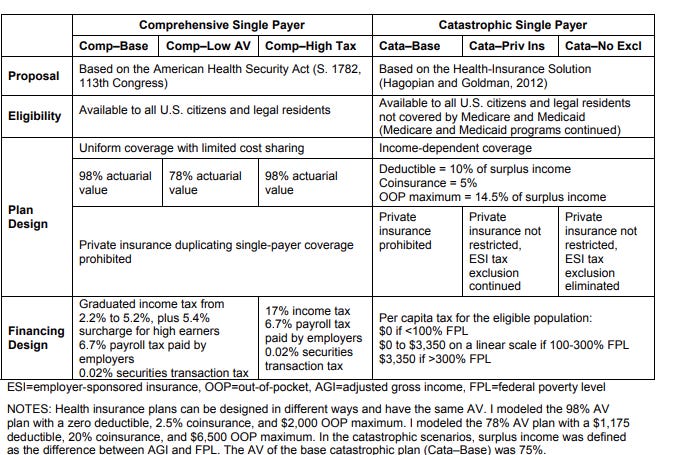
The results of the analysis? While national healthcare spending increased with the Sanders proposal (“Comp Base” in the chart below), it decreased in three different variations of the catastrophic plan.
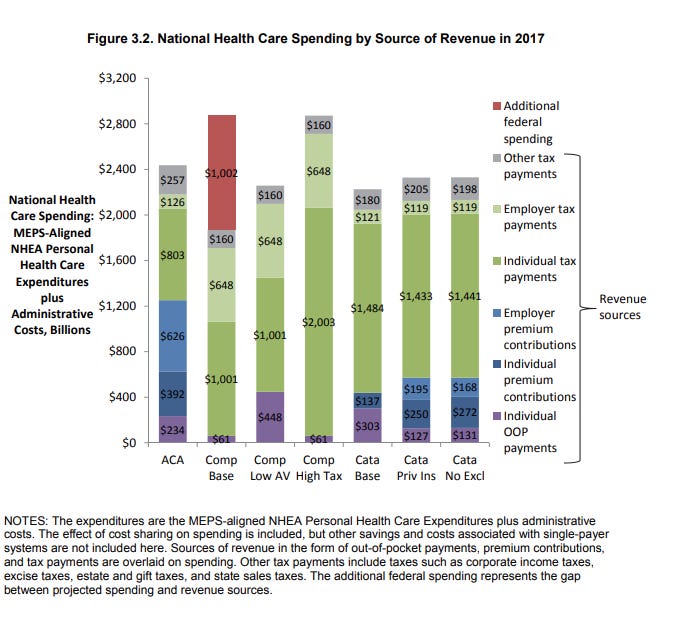
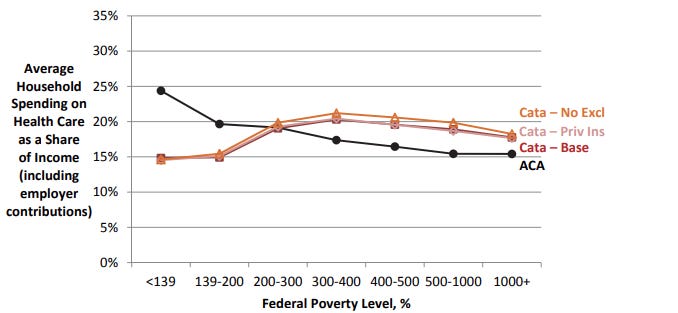
The catastrophic plan also had more equitable distribution of household spending on healthcare with the poorest Americans paying less that the current system and the wealthiest Americans paying a bit more.
One other advantage of the catastrophic coverage proposal is political: given that it could still allow employer-based insurance or other insurance coverage for the deductible, it would be less disruptive to the market, and may therefore be more politically feasible.
I don’t pretend to be a healthcare expert, but it seems to me that the Niskanen Center proposal offers the possibility of a reform that could be attractive to both the right and the left. The market approach to most health care would be attractive to the right, and the universal coverage would be attractive to the right. Once the current debate over the Obamacare subsidies is resolved, I hope we can have serious discussions about how to best improve our health care system.
Interesting. I would include within the options the ability of everyone to participate in Medicare, the so called single payer option. I would also largely prohibit PE acquisition of providers. Also worth looking at is the amount of costs attributable to private insurers.